
Pivot Extend®
Our permanent, flow-adaptive valve support for tricuspid regurgitation (TR)—
A permanent implant designed to restore coaptation and sustain heart function through dynamic, self-centering support.
Pivot Extend®
Device Summary: Pivot Extend®
Intended Use
Target Disease
TR Severity Treated
Target Population
Implant Duration
Deployment Method
Removal
Anchoring
Spacer Design
Spacer Materials
Valve Interaction
Flow Preservation
Adaptability
Procedural Setting
Customization
Definitive therapy for secondary tricuspid regurgitation
Secondary tricuspid regurgitation
TR inclusive of severe to torrential cases with a preference for massive to torrential TR
High-risk, frail, or inoperable patients with severe TR
Permanent
Transfemoral venous access / transcatheter
Removable and reversible by transcatheter retrieval
Atraumatic non-fixated anchoring (IVC + PA)
Self-centering oblong spacer with flow-adaptive saline-filled balloon
Nitinol mesh structure, fully encapsulated saline-filled balloon
Supports leaflet coaptation without fixation or leaflet trauma
Spacer designed for hemodynamic flow around the device
Dynamic self-centering and adaptable to progressive cardiac remodeling
Percutaneous intervention; cath lab or hybrid OR
Spacer volume can be adjusted during procedure to fit patient-specific valve anatomy (12mm~20mm dia.)
Pivot Extend® Delivery
Flexible, Transfemoral with In-Procedure Balloon Customization
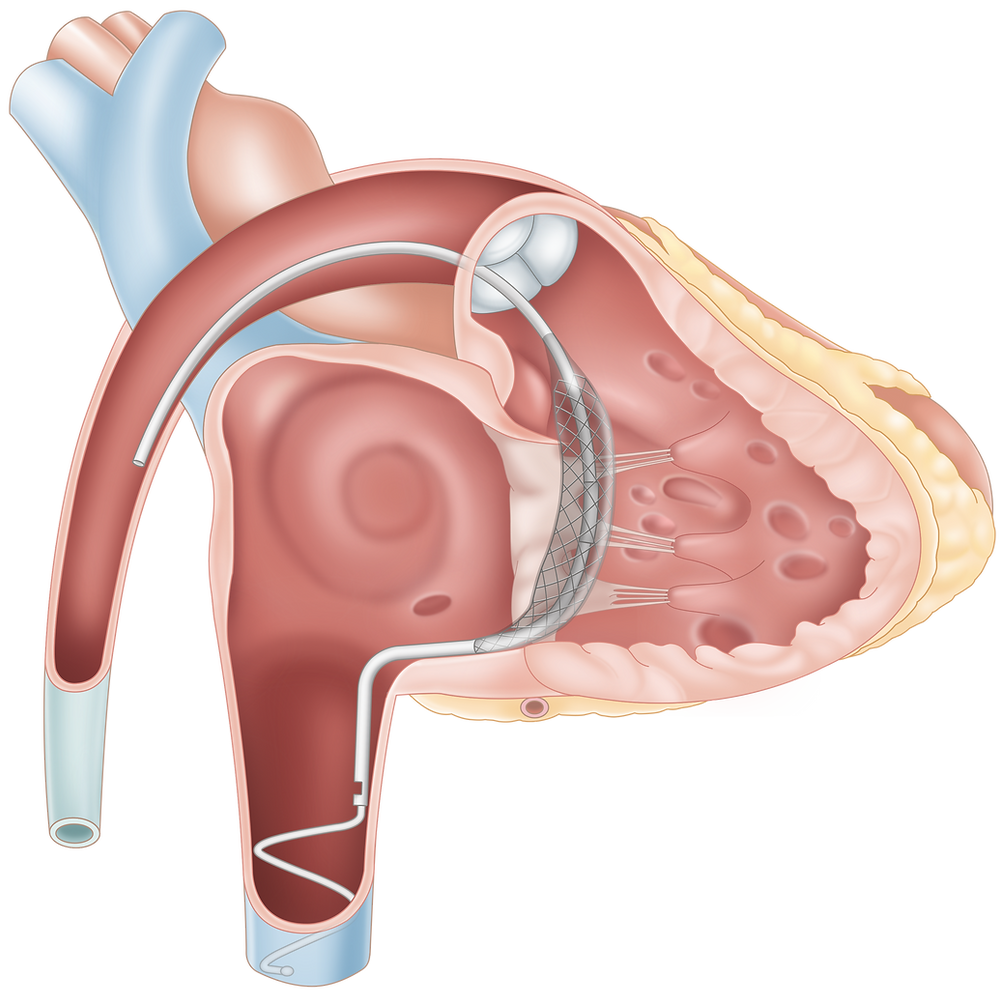
Pivot Extend® is delivered through a transfemoral vein catheter system, introduced via the IVC and advanced into the right atrium under standard fluoroscopic guidance. The implant is positioned so that the saline-filled balloon spacer spans the tricuspid valve in an oblique orientation, secured by non-fixated anchors in the IVC and PA.
Unlike traditional fixated systems, Pivot Extend® uses flow dynamics and device geometry to remain centered and stable. The balloon volume is adjustable during the procedure to match the patient’s valve anatomy, enabling customized coaptation. The system does not require TEE or ICE guidance and allows for catheter-based retrieval within 2–4 weeks if needed.
Access Site
Transfemoral venous access (standard percutaneous approach)
Delivery Path
Femoral vein → IVC → Right atrium → Pulmonary artery
Deployment Orientation
Oblique positioning across the tricuspid valve
Proximal Anchor
Distal Anchor
Spiral structure within the IVC
Atraumatic extension into the pulmonary artery
Spacer Design
Saline-filled balloon, Nitinol mesh support
Intra-Procedural Adjustment
Balloon volume is adjustable during implantation / Tailored to individual valve anatomy under fluoroscopic or echo guidance
Imaging
Fluoroscopy-guided, No TEE or ICE required
Retrievability
Fully catheter-retrievable within 2–4 weeks post-implantation
Est. Procedure Time
~60 minutes
Learning Curve
Low; designed for rapid adoption by interventional teams